What is gum disease?
Gum disease [periodontal disease] is disease within the supporting structures [gingiva, periodontal ligament, alveolar bone] that hold your teeth in your head [see basic anatomy].
It is the most common chronic inflammatory disease seen in humans.
In its severe form it is the 6th most common disease [people aged 15-99] in the world, affecting 10.8% of the world’s population some 743 million people [Global Burden of Disease Study 2010].
In the UK it affects approximately 45% of people with teeth [dentate] over 16yrs, with 37% mild, 7% moderate and 1% severe levels of disease [Adult Dental Health Survey 2009].
It is caused by accumulation of plaque due to inadequate oral hygiene. This starts it off and is responsible for its continuation.
It is often referred to as a ‘silent disease’ as to start with the patient is often completely unaware there is a problem and it isn’t until the disease is well established that the patient has symptoms that may prompt them to seek help.
In early stages of the disease the patient may experience bleeding of their gums, receding gums and bad breath [hopefully pointed out by a concerned friend or partner].
Eventually this progresses to loss of tissues that hold your teeth in your head [periodontium], tooth mobility, drifting and finally tooth loss.
In it’s early stages periodontal disease is a common preventable disease that can be treated a relatively low cost.
Like all diseases the earlier it is detected the greater the chance of successful treatment and the better the outcome for the patient.
Prevention is better, simpler, cheaper and less painful than cure!
Leaving aside one or two more specific gum conditions this section is all about ordinary ‘common or garden’ general gum disease which we can all get.
Gum disease or periodontal disease encompasses two conditions Gingivitis and Periodontitis.
Gingivitis.
In health your gums should be pink, stippled [a bit like orange peel], with a knife edge point of gum between your teeth [colour may vary due to ethnicity].
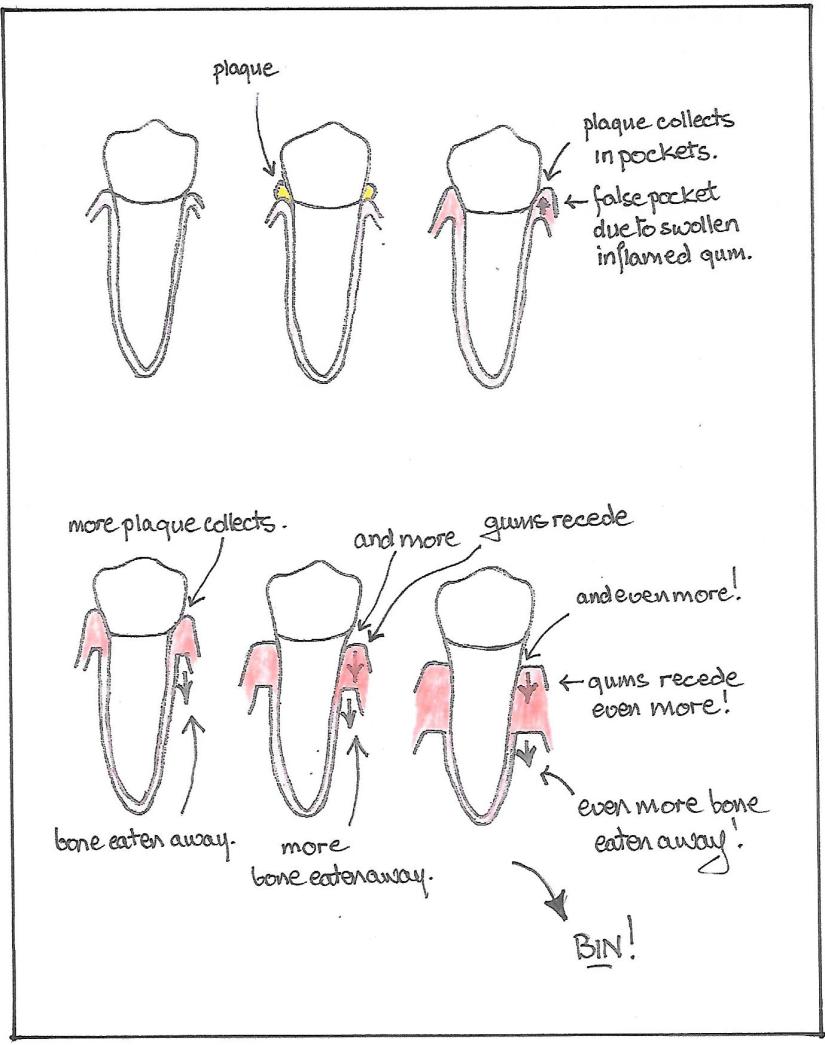
Think of your gum as a little windowsill around your tooth, plaque sits on this little window sill, bits of food debris stick to the plaque and little colony of bacterial plaque feed on these bits of food debris producing toxins as a by-product and they of course, multiply. The gum [gingiva] is a little collar around your tooth like a short tight polo neck [see basic anatomy]. The toxins make this little collar of gum irritated and inflamed and so it swells. So your little polo neck turns into a deeper polo neck and eventually into a floppy turtle neck.
The plaque on your teeth is the same bacterial plaque that causes caries [tooth decay] but no sugar is needed to cause gum disease. It is an NCD [non communicable disease], you don’t catch it from other people. The bacteria which cause it are endogenous, they live on you anyway. Which bacteria? Hundreds of different types and they are the ones we know about!
‘itis’ means inflammation as in tonsillitis, appendicitis etc. Thus Gingivitis is inflammation in the gingiva.
Behind your little collar of gum is a little gutter between the polo neck and your tooth, so an indication of how bad this infection is can be found by measuring the depth of the gutter, officially called a periodontal pocket.
Your dentist will do this with a special probe with marks on it called a periodontal probe. This probe also has a bobble on the end, so it only measures what’s there, it doesn’t make a hole!
In health this measurement should be 3mm and under [though I aim for all of my patients to have pockets under 2mm]. If your gums are inflamed and swollen this measurement will be bigger, this is called false pocketing. They will also bleed.
As the bacteria in the bottom of this pocket accumulate you start to get colonisation by more specialised bacteria that are able to survive without oxygen [anaerobic]. Inorganic ions in your saliva become incorporated into the plaque and the plaque hardens into calculus [tarter]. A bit like the fur in the bottom of your kettle.
This situation can be reversed by good oral hygiene. However while you can get on with the good oral hygiene you will also need to have a professional cleaning by a dentist, hygienist or therapist. Why? Because if you have a lot of calculus stuck on your teeth and in the little gutter around your teeth you will never with the best will in the world be able to get it off yourself and get your gums back to complete health. They will never be happy and healthy lying over bumpy calculus. A bit like trying to iron your shirt on a bumpy ironing board!
At this point this condition is reversible by hard work on your part and, with the help of your dental team, teaching yourself to clean your teeth effectively and efficiently. More to the point continuing to do so for ever!
You don’t have to clean all of your teeth- just the ones you want to keep!
Remember this little mantra- If they bleed they are sick, you need to clean them better!
Periodontitis.
If gingivitis is not treated by you with the help of your dental team, toxins produced by the bacteria build up in the bottom of the pocket and eventually begin soaking into the tissues through tiny micro ulcers [ulcer is a descriptive term meaning ‘a hole in your skin’].
From here they gradually destroy the little ligaments that hold your tooth in its bony socket and the pocket around your tooth deepens into what’s called a true periodontal pocket. This carries on going, creating deeper and deeper pockets allowing more plaque to collect and calculus to develop in the bottom of the pockets. Eventually the bone around your teeth is destroyed, your tooth becomes loose and is lost.
Thus periodontitis is a continuation of gingivitis.
Other Factors.
Now while periodontal disease is a bacterial plaque led disease there are other factors involved.
The factors involved in gum disease are;-
Genetics [for which you can cheerfully blame your parents], poor oral hygiene, smoking, undiagnosed or poorly managed diabetes and no doubt others we have yet to discover.
Do you know what genes you’ve got? Well I don’t and I’m too scared to risk it!
So if you have the wrong genes and you exacerbate that by poor oral hygiene and smoking you are stuffed as far as keeping your teeth is concerned!
A word here about smoking, apart from the fact that you know it’s a bad thing one of the problems for smokers is because the blood supply to their gums is reduced they don’t necessarily get bleeding and so they don’t pick up early signs of gum disease.
Where do you start?
Well as with any disease you need to start with discovering it, diagnosing it correctly, deciding if it’s limited to a few teeth in your mouth or all of them [localised or generalised], deciding how bad it is and forming a plan of action.
You can start by cleaning your teeth properly as well as you can.
Then you need to go to the dentist. One of the problems with gum disease is patients often don’t visit the dentist until they have a problem. With gum disease they might get bleeding, bad breath, a horrible taste in their mouth from pus or gasses given off by the bacteria, their teeth might be loose, moving around or painful. By this time things are well on their way.
The best way to deal with any disease is to stop it happening in the first place.
Prevention is better, simpler, cheaper and less painful than cure!
The time to go to the dentist is before you have problems, in fact before you have the disease in the first place. Your gum disease status should be checked every time you go for a check-up from when you are young so early indicators can be picked up, advice given, oral hygiene techniques taught and you are in good habits to prevent you getting gum disease in the first place.
BUT IT’S NEVER TOO LATE- GO NOW!
What will the dentist do?
Well they will do all of these things;- check your medical history, take a history of whatever is bothering you [a history as you say in medicine is the story in the patients words, what the problem is how long you’ve had it what makes it better/ worse etc], then they will probably ask you a whole load of questions about your problem and various other things such as your oral hygiene regime, check all of your teeth and restorations, look over your mouth and surrounding areas for any signs of oral cancer or any other conditions, MEASURE THE POCKETS AROUND YOUR TEETH WITH A PERIODONTAL PROBE, chart all these findings.
They may do various other ‘special tests’ which will probably include taking xrays [radiographs] if they do not have recent ones to refer to.
Then they will get it all together in their head and explain it all to you. I find visual aids very helpful for this, I draw little diagrams or use flip charts, some people may use little videos, all sorts. The dental team’s job is to explain to you, hopefully in a way that you will understand the overall condition of your mouth, all of it, holistically in keeping with the rest of your body. Then identify any problems they feel you have, explain what hopefully the solution is and what they would advise as a plan of action [this is called a care plan]. Let the dentist talk you through it in what they feel is a logical order. Most of us have a well rehearsed script which has all the information in it we feel is important. It’s very easy to get lost if the patient keeps interrupting all the time, listen first, then ask the questions. I usually stop every so often and ask the patient if they want me to repeat anything, I am sure your dentist will do the same, it’s no good charging ahead if the patient has got lost along the way.
Several things to say-
Answer all the questions as well as you can, if you can’t remember a sequence of events write it down.If you don’t tell them they won’t know!
If you are on any tablets or medicines and you can’t remember the names take a list or a copy of your latest prescription. If you have had a lot of operations or other complicated medical things write it down with approximate dates.
If you are worried, apprehensive, scared stiff, panicky, anything- say so. While experienced dentists are pretty good at reading body language even the most experienced of us get it wrong sometimes. Nobody minds, we’ve heard it all before, everybody is different, we all have things that upset us and worry us or we are scared off, don’t feel you have to pretend. I’ve had great big blokes cry all over me- I don’t think any the worse of them- it’s fine. IT WILL BE FINE. It’s a lot easier from my point of view to deal with someone if I know what worries them, your dentist has many skills but I doubt if telepathy is one of them. You can’t help a patient get over/ cope with their worries or fears if they don’t tell you what they are.
If you need to take someone for moral support- do so. No one minds.
If you don’t understand what the dentist is telling you, get them to say it again. All of us however intelligent we are when faced with something new, out of our field, unusual etc get confused. Get them to repeat it till you do understand it. Their role is to teach you how to look after your teeth and that starts with you, the patient understanding the problem. You’re not daft, it’s just new to you that’s all. Some treatments might have options, that will be explained to you and if you’re not sure- ask.
The dentist will give you an honest appraisal of the condition of your mouth and supporting structures [like a surveyor when you’re buying a house], they will advise you as to what they think a suitable care plan should be. When it has all been explained and you have asked any questions you might have, it’s up to you to think about it all and decide what you want to do. You are the patient, it’s your mouth. You have to decide, patients quite often ask me what I would do in the same circumstances and I always tell them but it’s still up to the individual to decide for themselves.
The dentists job is to look at the whole of your mouth and surrounding area as part of the rest of your body. The dentists job is not drilling holes in teeth! They will look at everything including what ever you feel is your problem which may not be what the dentist identifys as being your most important problem. The point of the care plan is to treat things in a logical order. That logical order starts with you being able to maintain your dentition properly with good oral hygiene and making sure your teeth are solidly in your head by tackling any gum disease issues first. As every builder knows the most important thing about a well built house is solid foundations, spend what you like on designer wallpaper but if your house is going to fall down there is no point!
But life gets in the way sometimes- diagnosis, plan of action, then what? The patient understands, they know what they need to do themselves and in terms of treatment. Then something happens- they are ill, they have a baby, their Mum dies, they lose their job, move house, split up with a partner just can’t hack it for some reason at the moment. Not in the right mind set. That’s OK we understand. As long as you understand we can’t change the rules of science, can’t change the diagnosis, the bugs don’t know what’s going on in your life and what’s more they don’t care either! But we do and we understand and one day when you feel better we will be there for you.
Further reading.
Don’t take my word for it, look up the British Society of Periodontology at www.bsperio.org.uk
Periodontology is the science of Gum Disease. It is a specialist subject within Dentistry. The society is ‘devoted to education and raising awareness within the dental and medical professions, students, patients and the general public of the importance of gum health for all ages’. Anyone can look up its resources and read the information. It has a very good patients section and you can down load and print things off including better info graphics than mine!
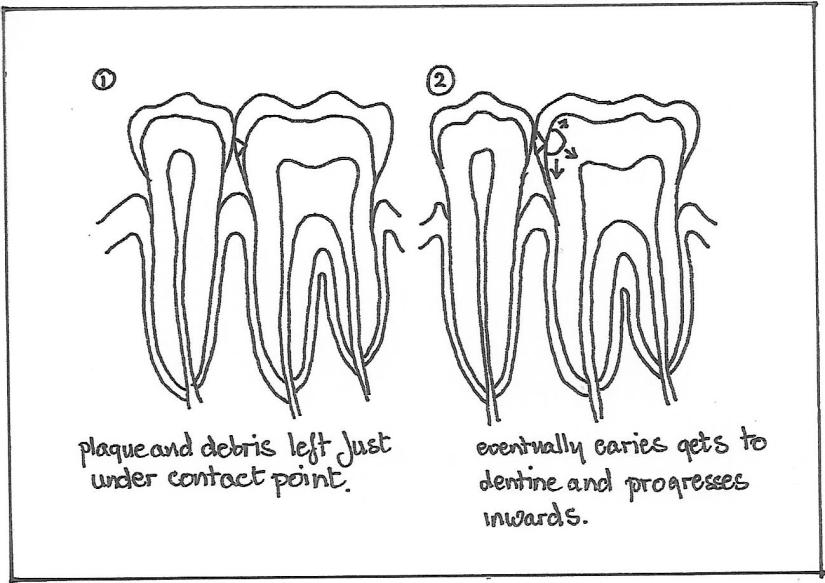
Diagrams.
Here few diagrams, I hope they are understandable gum disease is much easier to understand visually. I hope they are helpful.