So we will all get older, it’s inescapable.
If we have our teeth and want to keep our teeth it will require diligence, attention to detail and effort on our part to do so it won’t just happen by magic or luck!
No amount of going to the dentist and no amount of money is going to keep our teeth in our head unless we are prepared to do the day in, day out maintenance consistently, thoroughly and effectively. This includes perfect oral hygiene and attention to what we eat and drink.
So you do all that already [bravo] and you think that’s the whole story but there are certain things that happen as we age which you need to be aware of in order to keep on top of things;-
Eyesight.
So most of us get to a certain age and need reading glasses or you may always have needed glasses for near vision. Make sure you put your glasses on when you clean your teeth and do it in the mirror, you need to see what you are doing to clean your teeth effectively and efficiently. Good lighting is also essential, by the age of 60 we need 3x more light to be able to see detail than we did when we were younger.
A very useful source of information about light, sight and ageing eyesight can be found on The Serious Light website at www.seriousreaders.com they also give all the links to the relevant NHS information for conditions that affect your eyesight as you get older.
Dry Mouth.
So as we get older lots of us get a dry mouth [see chapter 11].
Our mouths are like a little sluice, saliva is constantly being made by our salivary glands and washing things down our throats. Saliva has a function.
It lubricates our mouths to make it comfortable to chew, swallow and speak properly. Some of our food needs to partially dissolve in saliva in order for us to taste it. It helps with immunity as it contains antibodies and other antimicrobials. It contains enzymes [alpha amylase in particular] which start digesting out food helping to ‘clear up the bits’. It helps in remineralising our enamel and it buffers the acid in our food and drink back to neutral to stop it dissolving away our teeth.
Saliva is a truly magical substance.
Leaving aside certain conditions the two commonest reasons for a dry mouth are our salivary glands being a little less efficient as we get older and polypharmacy.
Salivary Glands.
As we all get a bit older our salivary glands like other bits of us become a little less efficient. You have 3 major pairs of salivary glands; – parotids in front of your ears [swell up when you get mumps], sub mandibular underneath the angle of your jaw and sublingual under your tongue. These produce to different extents a mixture of mainly serous [watery] saliva and mucous [thicker saliva]. All over the inside of your mouth you have lots of little salivary glands within the skin of your mouth [oral mucosa][a bit like the sebaceous glands in your hair], these make mucous.
Poly Pharmacy.
So as we all get older some of us are on drugs for various conditions and as we are living longer more and more people are living with medical conditions [co- morbidities] that 50 or so years ago we would not have been living with because we may not have lived long enough to get them! [Not to mention non-communicable diseases / life- style conditions such as diabetes type 2]. Some of the drugs for these conditions cause dry mouth, the commonest ones are the ‘antis’;- antihistamines, antihypertensives [high blood pressure] and some anti-depressants, plus loads of others.
So if you are producing less saliva for whatever reason, you are not constantly washing, remineralising etc your teeth and so you will become INCREASINGLY SUSCEPTIBLE TO CARIES [TOOTH DECAY] AS YOU GET OLDER!
Something which may help you if you suffer with a dry mouth at night are Xylimelts. These are naturally adhering discs that you stick to your gum above your top back teeth, they deliver time released xylitol, so stimulating saliva production. Available from www.mouthulcers.co.uk . You can buy a trial pack for £1 so you can’t go wrong!
Manual Dexterity.
As we get older we may get a bit of osteo arthritis in our hands, lots of other conditions may make us less manually dexterous, or you may have had something like a stroke on a side of your brain that means you have lost/ reduced use of your dominant hand. This of course means you have to start learning to clean your teeth all over again at a ripe age with the wrong hand. Not easy at all!
An electric toothbrush can be very helpful in these circumstances. I would choose a round headed one for preference as it is the same shape as the surface you are trying to clean, namely the gum margin around your tooth where bacteria like to lodge [see below]. Whatever brand you choose you do not need to by the fancy expensive model to start with, just buy the basic one that is perfectly good enough. Then if you find you get on with it you could update to a newer model in the future [keep the old one for holidays it’s bound to be your nice new expensive one you leave in a hotel room or campsite somewhere!] You will find with an electric toothbrush that it starts to loose it’s oomph after 5 years or so, so you can buy an updated one then.
There are also lots of gadgets and toothbrush designs to help those with problems gripping a toothbrush. Ask your dentist or hygienist for help that is what they are there for- to help you take care of your teeth.
I myself keep a big box of samples of such things that I have been given by various dental companies to try out on my patients. I am sure other dentists do the same. If it works for you it may help another with similar problems. You have the problem, our job is to try and help you achieve your desired solution- to be able to clean your teeth effectively, thoroughly and efficiently.
Forgetfulness.
Well this happens. If we are not looking for our glasses we are trying to remember what we were looking for! We don’t lose our memory we lose our recall- not the same thing.
Dementia sufferers have even more problems.
Reduceable/ treatable [reversible] causes of dementia include;- drug and alcohol misuse, emotional illnesses such as depression, some metabolic disorders, endocrine disorders [glandular], nutritional deficiencies [especially B vitamins], trauma to the brain, some infections and arteriosclerosis [plaques of debris sticking to the inside of the blood vessels] of the blood vessels in our brains.
Irreversible dementia includes Alzheimer’s disease [about 70% of cases in the UK], vascular dementia [20%] and lots of other rarer types [10%].
More and more people are being diagnosed with dementia due to better diagnosis, we are also living long enough to get it and of course it ranges in severity from one patient to another.
If this is you or a loved one it is very important that you have a good oral hygiene regime, so it’s ingrained in your psyche- put instructions to yourself up on the bathroom mirror, put the bottle of mouthwash on the loo cistern so when you go for a wee after lunch you see it and it reminds you.
Dental teams are becoming more and more adept/ aware of the problems facing people who have dementia as regards their oral health. They are there to help you. If you have a carer or relative who helps you with personal care it’s not a bad idea to take them with you to your appointments so they can get advice from a professional and understand how they may help you.
THERE IS NO SUBSTITUTE FOR PROFESSIONAL HELP TAILORED TO THE INDIVIDUAL!
Here are some things you need to be particularly aware of;
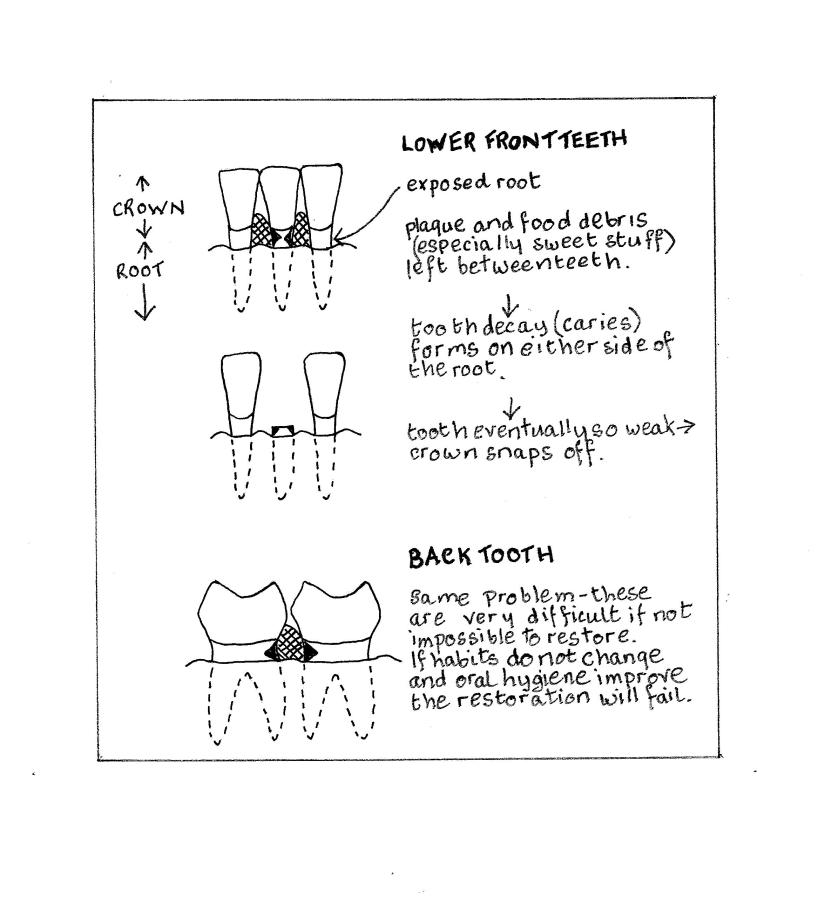
1- Root caries.
As we get a little older some of us start to show our roots. The crown [the top portion of our tooth] is covered in nice hard impervious enamel but our roots are not. They are covered in cementum which is quite soft and is probably brushed off in the first year it is exposed. So we are left with bare dentine which is more susceptible to decay [caries].
The dentine is not prone to decay, prone is- ‘she forgets to put her glasses on so is prone to walking into lamp posts’, no your dentine is susceptible to caries underneath any plaque you may leave on it.
Prone and susceptible are not the same thing.
If you leave plaque on your roots you will get decay under that plaque. The bacteria in the plaque will metabolise the sugar in your diet producing acid which causes caries. The plaque sits on the little window sill of gum around your tooth and in-between your teeth so these are the areas that need particular attention when you clean.
Your teeth need to be cleaned regularly, effectively, efficiently and thoroughly.
The factor you can’t do anything about is reduced saliva flow but you can ensure that you keep yourself hydrated [1.5 litres of fluid per day for a woman and 2 litres for a man], you can chew sugarless chewing gum after eating to encourage the flow of saliva.
You need to eat a healthy diet with plenty of fresh fruit and vegetables [at least 3 veg and 2 fruit] with as little refined sugar as possible. Any sugar eaten should be eaten with a meal and not constantly snacked upon, the amount and the frequency are equally as important.
If you have a lot of exposed roots, especially if you have reduced salivary flow your dentist may prescribe high dose fluoride toothpaste, to use on your little brushes in-between your teeth and perhaps to clean all of your teeth. This is a prescription only medicine [POM] and like all prescribed medicines only to be used by the person it is intended for. It is not for use by all the family and should be kept out of reach of small children and other vulnerable people.
If you have early decay on your roots you may also be prescribed this medicine as it is better for the health of your tooth to treat this problem medically by stopping [arresting] the caries from progressing by cleaning and ‘medicating’ with fluoride than drilling a hole in your tooth which will weaken its structure.
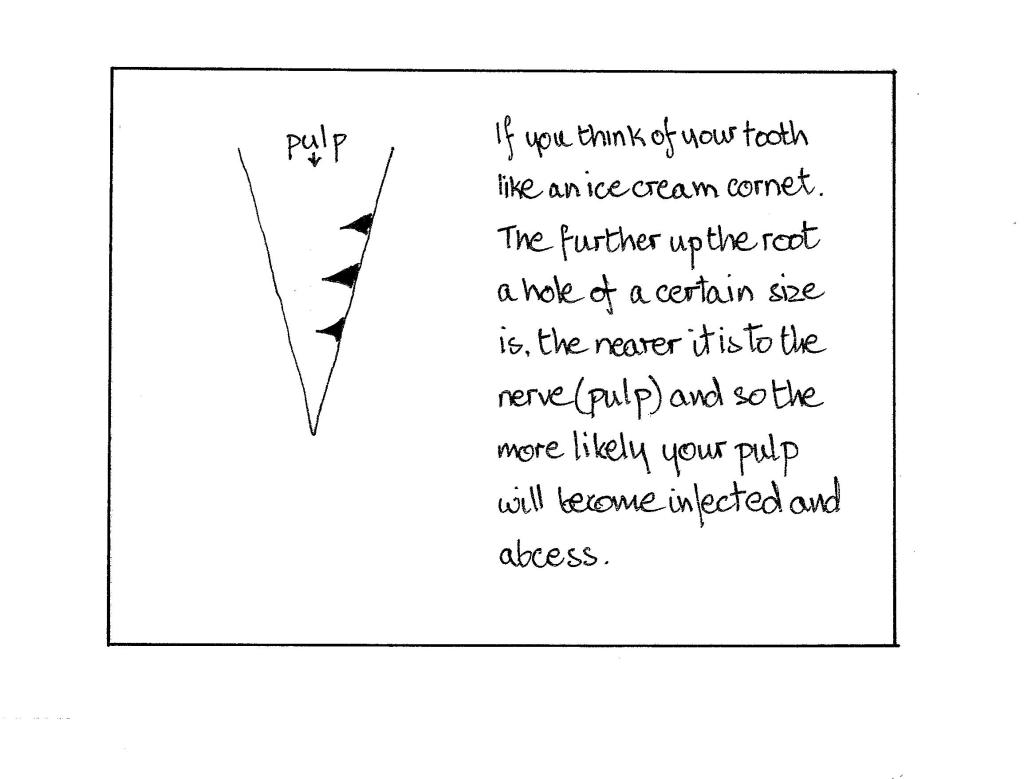
Time for a couple of little diagrams-
2- Before or after breakfast.
So should you clean your teeth before or after breakfast? This is always a subject of debate within the dental profession.
Here is the theory; – if all the bacteria [that have grown over night] are removed from your teeth before breakfast then, in theory it shouldn’t matter how much sugar you eat for breakfast there will be no bacteria to metabolise it into acid.
This all sounds wonderful and logical BUT theory is all very well, doesn’t always work in practice. For a start no one is a perfect cleaner [though that is no excuse for you not to strive for perfection!]. Secondly if you are a person with great big gaps in-between your teeth you are going to leave toast and marmalade/croissant/ raisons in-between your teeth which is not going to get brushed off/ washed out ‘till lunchtime, when more will be added!
So I would say do your whole cleaning routine before breakfast and then use your little brushes and give them a once over again with your toothbrush after breakfast and the same after lunch.
Research also shows that 3x oral hygiene per day reduces your risk of heart and other non-communicable diseases [NCDs], as it reduces the risk of gum [periodontal] disease, a chronic inflammatory condition. If your gums are inflamed and infected they will bleed, if the blood can leak out, the bacteria can leak in and so can be carried around in your blood system to settle in places it would be better they didn’t!
3- Denture health and cleanliness.
This is covered in the next chapter number 27.
